Neonatal Care Cases – Part 3

Umbilical Vein Catheter Placement – More Safety with POCUS
In today's blog, we'll delve into the importance of using Point-of-Care Ultrasound (POCUS) in the Neonatal Intensive Care Unit (NICU) by presenting a real patient case who needed umbilical vein catheterization. This procedure is often employed for vascular access in newborns when other types of venous access are difficult to obtain. We'll explore the significance of proper placement, the role of POCUS, and the complications associated with malpositioned umbilical vein catheters (UVCs).
About the technique:
Umbilical vein catheterization involves the insertion of a catheter through the umbilical stump, providing venous access through the umbilical vein. This procedure allows direct medication, fluids, and nutrition administration while facilitating continuous blood gas and pressure monitoring. The UVC remains viable for up to 14 days after birth. Conversely, the umbilical artery catheter (UAC) is inserted into the arterial system of the umbilical stump, used less frequently but necessary for monitoring, blood sampling, and administering specific fluids.
Patient case
A three-day-old female neonate, Gestational Age at Birth: 28 weeks, Birth Weight: 1,100 grams, was born prematurely via emergency cesarean section due to maternal preeclampsia. She required immediate respiratory support for respiratory distress syndrome (RDS) and was admitted to the NICU. A central line was established through an umbilical artery catheter to monitor blood gas, and shortly after that, an umbilical vein catheter (UVC) was placed to provide better venous access for medications and fluids while reducing the need for multiple peripheral intravenous lines.
X-ray
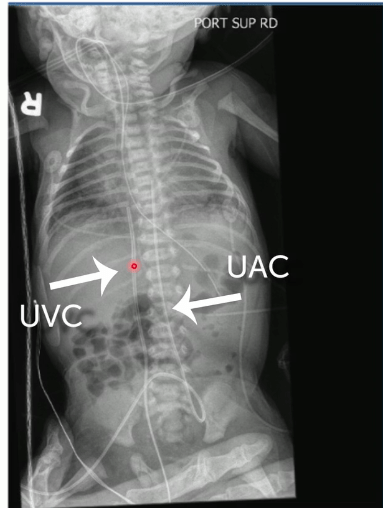
Upon initial insertion, an x-ray was taken to confirm the correct placement of the UVC and the UAC. Can you distinguish between the UVC and UAC in an X-ray, and are they correctly positioned?
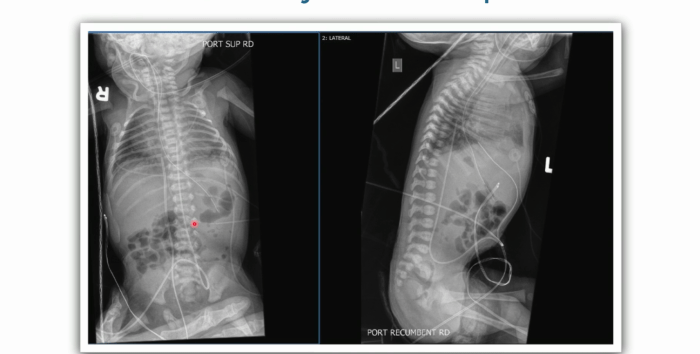
Is everything in the right place? In this X-ray image, the catheters look correctly positioned. In the following, however, you will see that taking a second look with ultrasound is advisable.
Where is the UVC tip?
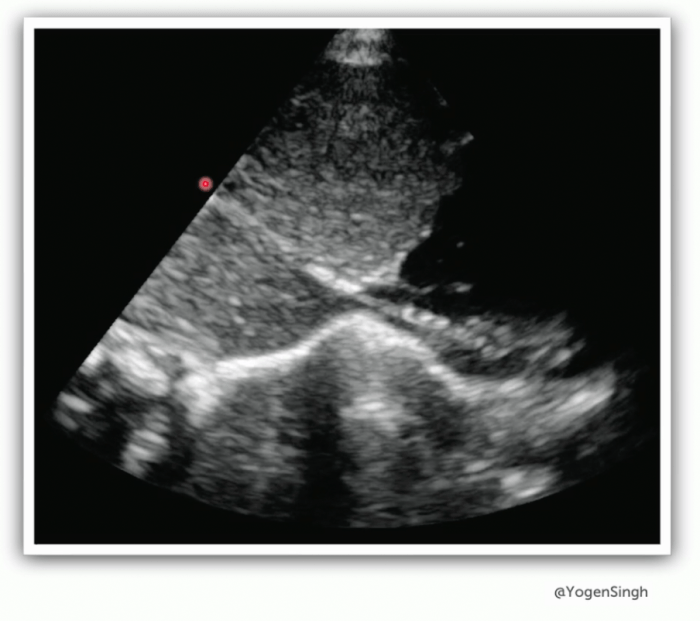
An echocardiogram is performed eight hours after initial placement for a different reason. Look at the following ultrasound image. Can you spot the UVC tip?
Conclusion
In this case, the UVC tube was placed too deep. The ultrasound picture shows how it travels through the Ductus Venosus into the Inferior Vena Cava before reaching the heart. It then moved through the Foramen Ovale and ended up in the left atrium. On the original echo loop, you could see the UVC tip lying in a pulmonary vein.
There are two possibilities as to what happened: first, the UVC could have been malpositioned despite the initial X-ray indicating correct positioning (we know that ultrasound does a better job in this regard than X-rays). Second, the UVC could have migrated in the last 8 hours. Subsequently, the UVC position was corrected and confirmed with POCUS.
What is generally considered the ideal position for the UVC tip in neonatal care?
A) In the left atrium of the heart.
B) In the right atrium, right after the IVC enters the heart.
C) In the inferior vena cava, just above the diaphragm and below the heart's right atrium.
D) At the IVC-portal vein junction.
Correct Answer: C) Ideally in the inferior vena cava, just above the diaphragm and below the heart's right atrium.
Explanation: The subdiaphragmatic vestibule (SDV) is the region right above the diaphragm and below the right atrium. It is the specific region where the UVC tip should ideally be placed. This position ensures proper delivery of fluids and medications while minimizing complications.
Pitfalls in UVC Catheter Placement
UVC placement is challenging; complications can occur in roughly 20% of patients. Malpositioning is the most common problem, followed by infections. Malpositioning, in particular, presents significant issues, such as a high infection rate, thrombus formation risk, and the potential for severe consequences like stroke or pulmonary embolism due to thrombus formation. In addition, malposition can lead to perforation, hemorrhage, and abscess formation in the liver, cardiac arrhythmias, and cardiac tamponade.
A common factor that increases the risk of malposition is gestational age. ELGAN (Extremely Low Gestational Age Newborns) may present with substantial differences in size and general anatomy of the venous system. In-depth knowledge of the anatomy is therefore vital.
Bringing ultrasound into the game
Ultrasound is pivotal in reducing the risk of UVC malposition and associated complications. It allows real-time visualization of the catheter's path and tip during insertion, confirming correct advancement through the umbilical vein and into the inferior vena cava. This immediate feedback minimizes the risk of complications and ensures proper placement.
Moreover, ultrasound is a safer alternative to X-ray, reducing radiation exposure, which is especially crucial for fragile neonates. Even when initial X-rays confirm correct placement, ultrasound can verify that the catheter remains in its intended position, as UVCs can migrate due to the umbilical cord's natural shrinkage.
Take-Home Messages
- POCUS is superior to X-ray for confirming UVC tip position.
- Follow-up ultrasound is essential because UVCs can migrate over time.
- Secure catheter fixation is crucial to prevent displacement.
- Ultrasound limits radiation exposure conserves resources, and saves time and staff.
- Proper training is necessary for UVC placement assessment with ultrasound.
In conclusion, POCUS is an invaluable tool in neonatal care, ensuring the safe and accurate placement of UVCs and reducing the risk of complications associated with misplacement. Its real-time imaging capabilities enhance the quality of care for fragile newborns, contributing to improved outcomes.
Learn to solve cases like this!
Did you know that we have many more such cases in our Neonatal & Pediatric Ultrasound BachelorClass? Learn more in our course – right now you can get it for -30% and Lifetime Access! But only until October 22nd! So be quick and get the Neonatal & Pediatric Ultrasound BachelorClass today!
GET COURSE