Abdominal US outperforms AR for NEC diagnosis

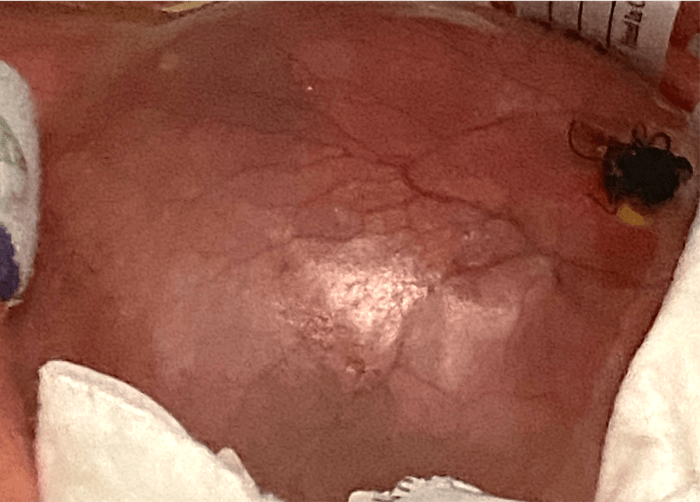
A preterm infant presented with a new onset of emesis and bloody stool. This picture showed the infant with a distended, discolored abdomen, which may be the manifestation of a life-threatening intra-abdominal process. The differential diagnosis included necrotizing enterocolitis (NEC).
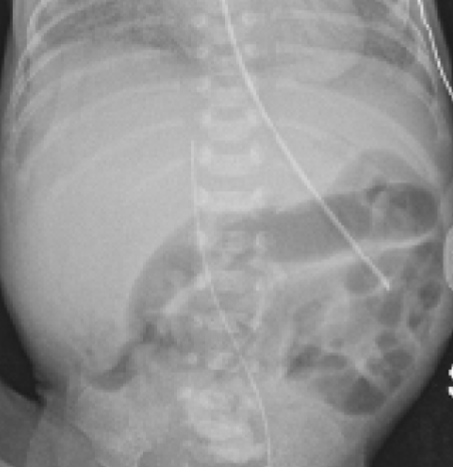
The abdominal X-ray (AR) showed a non-specific dilated bowel gas pattern.
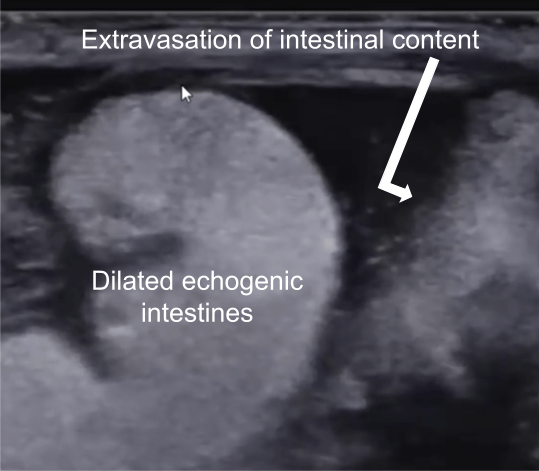
Abdominal ultrasound (AUS) was obtained. The intestinal content spillage from the intestinal perforation was "caught on camera." It also showed abnormally dilated, echogenic intestines. These findings were undetectable by AR alone.
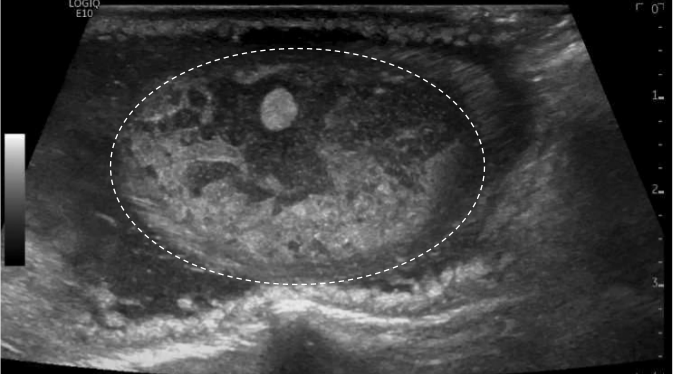
AUS also showed an extraluminal abscess and meconium collection. All these findings were consistent with NEC with intestinal perforation. This patient underwent emergent abdominal surgery for bowel resection and ileostomy.
1Chen, J., Mu, F., Gao, K. et al. Value of abdominal ultrasonography in predicting intestinal resection for premature infants with necrotizing enterocolitis. BMC Gastroenterol. 2022;22, 524. https://doi.org/10.1186/s12876-022-02607-0
2Cuna AC, Reddy N, Robinson AL, Chan SS. Bowel ultrasound for predicting surgical management of necrotizing enterocolitis: a systematic review and meta-analysis. Pediatr Radiol. 2018;48(5):658-666. doi:10.1007/s00247-017-4056-x
529 €
instead of 790 €!
Make sure to benefit from the offer before it's too late!
BUY COURSE